In 2018, the US recorded the first reduction in overdose mortality in over 20 years. This reduction in deaths was the primary driver of the first increase in measured life expectancy in years. Unfortunately, that was not the beginning of a new trend. Overdose deaths again increased in 2019, setting a new all-time record. However, the increase was much slower than in previous years and largely represents a plateau in overdose deaths between 2017 and 2019 even as preliminary data for 2020 suggests that overdose deaths have again begun to increase dramatically. Below are five key takeaways from the 2019 CDC overdose mortality data and our interactive overdose mortality dashboard.
- Overdose deaths remain at an unprecedented high, largely as a result of the rapid spread of fentanyl that began in the mid-2010s.
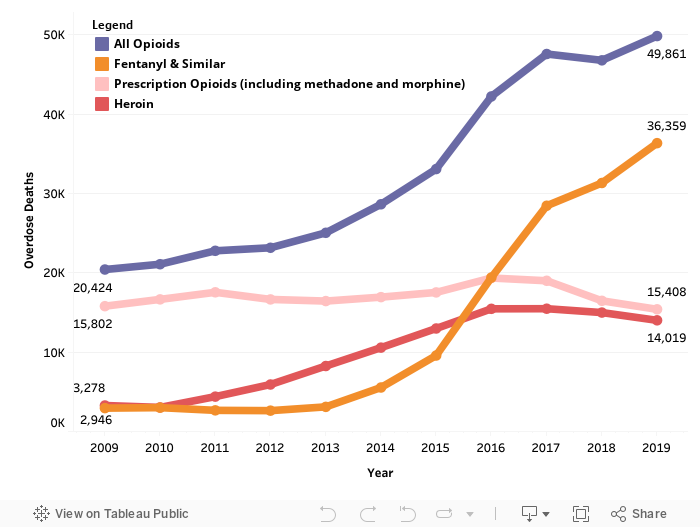
Overdose deaths have been steadily increasing for the last 20 years with the exception of a slight downturn in 2018. The number of deaths in 2018, however, was still higher than any other year in history except 2017 and now 2019. Beginning in 2016, the pace of overdose deaths accelerated primarily as a result of the substantial increase in overdose deaths that involve fentanyl or similar synthetic opioids. Overdoses involving fentanyl more than doubled between 2015 and 2016 from 9,580 to 19,413 and have continued to increase every year since hitting a new high of 36,359 in 2019.
Fentanyl is a synthetic opioid that was designed to treat extremely severe pain like that associated with advanced and terminal cancer. Because it is synthetic and strong (50 to 100 times more potent than morphine), extremely small amounts can replace much larger doses of traditional prescription opioids or heroin making it easier to traffic. For the same reason, it is particularly lethal and even trace amounts can result in overdose deaths. Fentanyl is also relatively cheap and may be mixed in with other drugs or used to manufacture counterfeit prescription opioid pills, which results in users ingesting more than they intended.
- An increasing number of overdose deaths involve stimulants—like methamphetamine and cocaine—whose lethality has increased due to intentional mixing and unintentional adulteration with opioids.
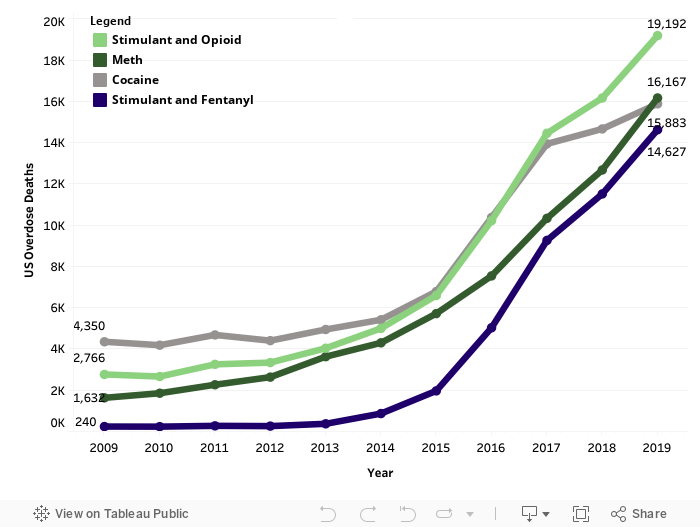
We have previously done deep dives into the dynamics of the increased mortality of methamphetamine and cocaine. In 2019 overdoses involving the two drugs remain at unprecedented peaks. Cocaine is most associated with the spread of solid or “crack” cocaine in the 1980s, and meth with the spread of the homemade version of the drug in the early 2000s that resulted in federal laws limiting sales of precursor chemicals including pseudoephedrine decongestant medication. The opioid epidemic’s dominance of the news for the past 10 years may make meth and cocaine seem like drug epidemics from the past but that is far from the truth. Overdose deaths associated with a stimulant (usually meth or cocaine) have increased four-fold over the past 10 years and the pace accelerated dramatically in 2016 with the introduction of fentanyl (an opioid). Before 2016 there were virtually no overdose deaths involving both a stimulant and fentanyl, but in 2019 there were 14,627. Fentanyl accounted for nearly half of stimulant related overdose deaths, while opioids of any type were involved in almost two thirds of stimulant related overdose deaths.
The uptick in these opioid & stimulant deaths is driven in part by the lethality of fentanyl itself—any use of a drug that has been adulterated with fentanyl is more dangerous than using that drug in a purer form—not only due to its physiological effects, but also because stimulant users may not be prepared to treat an opioid overdose. If administered quickly the drug naloxone can stop and reverse an opioid overdose to save someone’s life, but the drug has no effect on a stimulant overdose, so stimulant users may be less likely to carry naloxone.
- While both methamphetamine and cocaine deaths are on the rise, which drug dominates depends largely on geography.
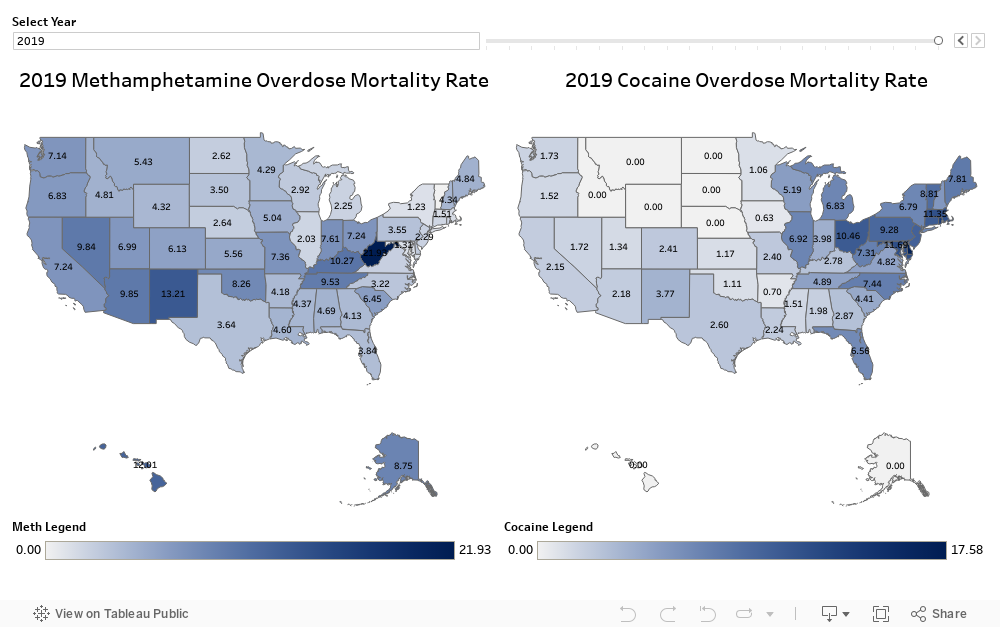
Methamphetamine is a drug that is traditionally associated with the Southwest, including New Mexico, Arizona, and Nevada, and that is where meth involved mortality was still highest in 2019. Cocaine, in contrast, is dominant in the Northeast states and mortality is particularly high in Rhode Island, Delaware, Maryland, and Washington, DC. Both drugs have also begun to spread from their traditional locations. Cocaine in particular has spread through the Great Lakes states including Michigan and Ohio and down the East Coast to Florida. Meth has also migrated, moving up the West Coast through California and into the lower Midwest and Appalachia. West Virginia currently has the highest meth overdose mortality rate in the country at 22 deaths per 100,000 residents. Many of the states that have most recently seen increases in meth overdose mortality were also states hard hit by the opioid epidemic. Ohio stands out as a state with both a relatively high meth overdose mortality rate and cocaine overdose mortality rate.
- The overdose epidemic is not solely a rural epidemic. Overdose deaths have increased and remain high for both rural and urban/suburban areas.
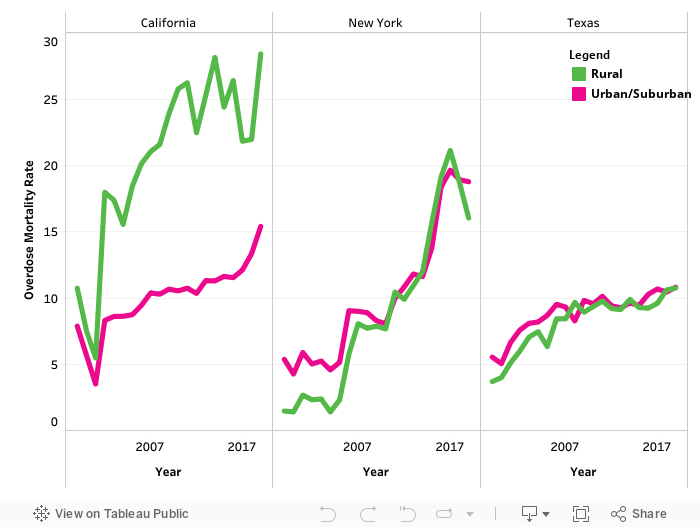
Overdose mortality is not just a rural or an urban problem—it is something that has affected all types of communities. The CDC categorizes all US counties by their urbanicity. Counties can be classified as rural or urban/suburban which allows us to calculate the rural overdose mortality rate and the urban/suburban overdose mortality rate for a state. In New York, for example, the trends, but not levels, in urban/suburban and rural counties have closely mirrored each other for many years. Until about 2009 rural counties had lower rates of overdose mortality than other counties but then rates equalized until 2019. Both rural and other counties saw a decrease in overdose mortality in 2018 but rural counties continued that decrease in 2019 whereas other counties saw an increase.
The patterns are slightly different for the US’s other two most populous states—California and Texas. Like New York, rural and urban/suburban counties in Texas have had both similar levels and patterns of overdose mortality but Texas did not experience the extreme spike in 2017 deaths that New York did, nor the decrease in deaths in 2018. California, in contrast, has vastly different patterns and levels of mortality between rural and urban/suburban counties. The urban/suburban mortality rate is on par with patterns in Texas—with a mortality rate between 10 and 15 per 100,000 but rural mortality is much higher beginning in 2002. By 2019 overdose mortality in rural California counties had spiked to nearly 30 per 100,000—twice the rate of mortality in urban/suburban counties.
- Overdose deaths affect all Americans but different racial and ethnic groups may be more affected by certain drugs than others.
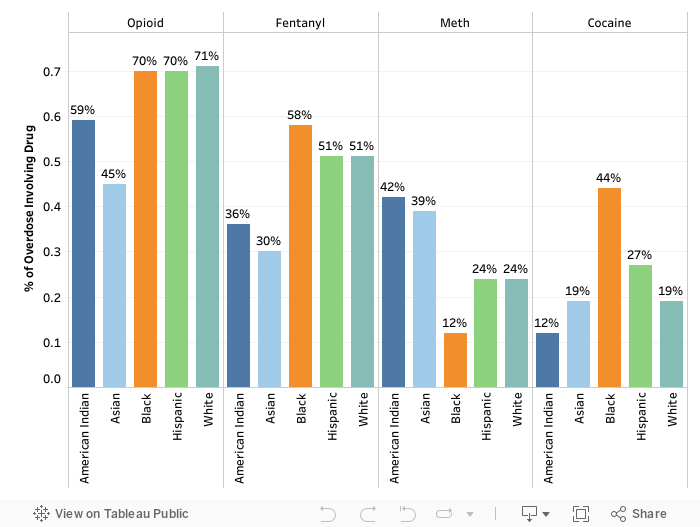
The overdose crisis is not confined to any one racial or ethnic group. Black and white Americans die from overdoses at similar rates. According to the CDC, in 2019 the age-adjusted drug overdose mortality rate for white Americans was 26 deaths per 100,000 only slightly higher than the rate for Black Americans of 25 deaths per 100,000. Hispanic and Asian Americans have lower rates of overdose morality—13 and 3 deaths per 100,000 respectively—and American Indians and Alaska Native populations have a higher rate at 31 deaths per 100,000.
For both Black and white Americans opioids continue to be the main cause of overdose deaths. 71 percent of white overdose deaths and 70 percent of Black overdose deaths involve an opioid of any type and 51 percent of white deaths and 58 percent of Black deaths involve fentanyl specifically. Both also have substantial stimulant related deaths, although more overdose deaths of Black Americans (44 percent) than white Americans (19 percent) involve cocaine, and more deaths of white Americans (24 percent) than Black Americans (12 percent) involve methamphetamine. Notably, Asian American and American Indian populations are most likely to be affected by meth with 39 percent of Asian American overdose deaths and 42 percent of American Indian overdose deaths involving meth.
Going Forward
The most important lesson from our 2019 overdose mortality dashboard is that the overdose epidemic remains pervasive in the US and is not limited to a single group, location, or drug. While much of the focus has been on the opioid crisis, deaths involving stimulants, especially stimulants adulterated with the synthetic opioid fentanyl, are on the rise. Fentanyl and similar synthetic opioids remain the primary drivers of our current historically high levels of overdose mortality. Reducing overdose mortality requires coordinated efforts by researchers, medical and public health professionals, and policy makers to treat addiction and promote harm reduction strategies. The COVID-19 pandemic has further complicated the public health response to the overdose epidemic and practitioners are developing new and creative strategies to confront this epidemic in a pandemic.
ABOUT THE AUTHOR
Leigh Wedenoja is senior policy analyst the Rockefeller Institute of Government