
On October 17, a new Food and Drug Administration (FDA) rule on hearing aids went into effect. This FDA action creates a new regulatory category of over-the-counter (OTC) hearing aids that will be available without a prescription, which people can buy directly.
The rule has been several years in the making. As part of the FDA Reauthorization Act of 2017, the FDA was directed to develop a category for OTC hearing aids for adults with mild to moderate hearing loss. As part of this process, the FDA used rulemaking procedures in the fall of 2021. The final rule (officially 87 FR 50698), released on August 17, 2022, went into effect this month. Proponents argue that OTC aids will increase access and affordability for millions. But the story of hearing aid access and use in the US is much older, and more complicated, than the five years of this rulemaking process. And, critics argue that this new rule won’t solve the structural issues that have created such a disconnect between need and use.
The Gap between Need and Access
Hearing aids are assistive devices that make sounds louder, and there are many different kinds used by people with a wide range of hearing levels. Proponents of the rule argue that the policy is much needed. An estimated 15 percent of US adults self-report as having trouble hearing. Specifically, the National Institutes of Health (NIH) estimates that 28.8 million Americans could benefit from using hearing aids, based on their hearing levels. Globally, the World Health Organization (WHO) estimates that disabling hearing loss impacts 466 million adults. Moreover, the number of people with hearing loss in the US and worldwide is expected to increase significantly, potentially doubling in prevalence in the US to over 73 million adults by 2060 as the population ages.
Despite the millions of Americans who may benefit from hearing aids, actual use is low. According to estimates from the US federal government, fewer than one third of US adults over 70 who would benefit from hearing aids have ever used one and the number is even lower for younger adults who would benefit. Most older adults report they have not gotten their hearing tested in the past decade. And even for older adults who have been given a referral by a doctor, one third reported not pursuing needed hearing-related healthcare.
Part of the reason may be cost. Hearing aids are expensive—estimates are that each hearing aid can cost $1000-$4000. That’s just for one. If a person wants or needs one for each ear, it’s double the expense. And while it’s not necessarily surprising that the technologies are expensive, what may be surprising is that health insurance largely does not cover hearing aids. This is not a recent development. Dr. Jaipreet Virdi, a deaf historian of science and technology whose research and writing often includes the history of hearing aid design and marketing, recently wrote about the decades-long history of the US classifying hearing aids as consumer, rather than medical, devices. Additionally, audiologists, healthcare workers whose specialization includes diagnosing and treating hearing and hearing loss, are not classified as medical professionals. This has meant that US health insurance plans often don’t cover their services. Dr. Arrianna Marie Planey, a health and medical geographer whose research focuses on health care access and equity, has argued that these political and economic dimensions have shaped who gets access and where.
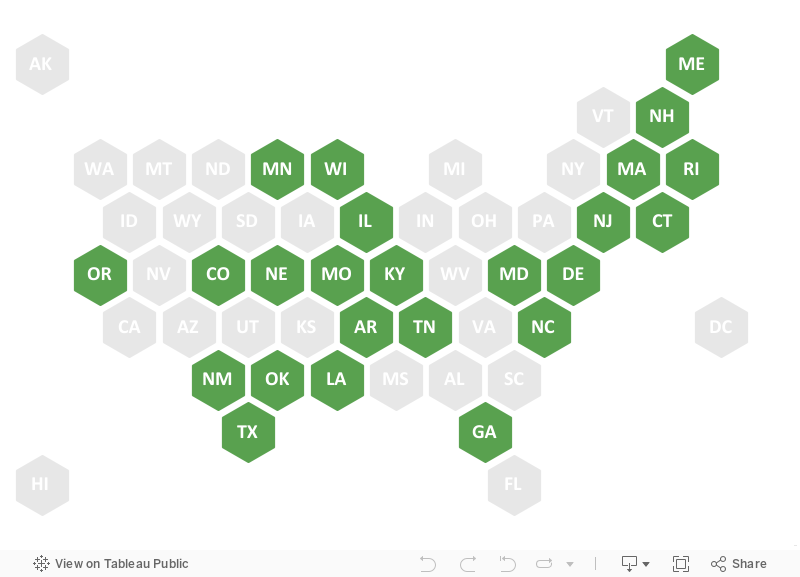
Classifying audiologists and hearing aids as outside of medicine has contributed to both hearing aids and related hearing healthcare not being included as essential health benefits in health insurance plans. If and how states require hearing aids to be covered by health insurance varies significantly. Many states do not require plans to cover hearing aids at all, including New York, and many other states only cover hearing assistive technology for children, not adults. Across the US, Medicare does not currently cover hearing aids or exams to fit them. Medicaid coverage of hearing aids does include children nationally, but again there is wide variation for adult Medicaid coverage by state. For example, Alabama has no covered services, whereas California does cover hearing aids (but not the batteries) if prescribed and supplied by authorized retailers.
Hearing Aid Requirements under State Health Insurance Laws
Coverage of Hearing Aids and Related Services through Medicaid
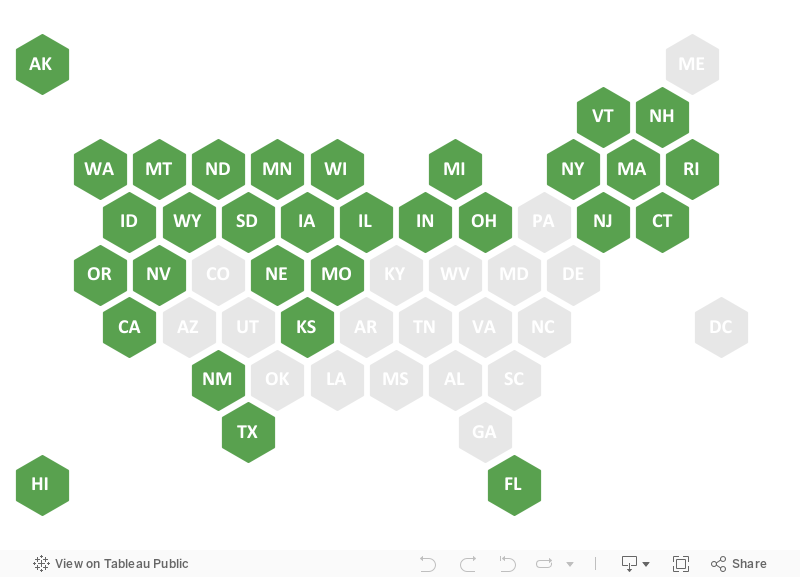
Data on state health insurance laws and Medicaid come from the Hearing Loss Association of America.
The changes to health care coverage and plans in the US from the Affordable Care Act (ACA) have not significantly changed insurance coverage either. The ACA doesn’t prohibit coverage but it doesn’t require it either. If and how healthcare plans created under the ACA include hearing aids also varies widely by state, according to data compiled by the Hearing Loss Association of America. For example, hearing aids are not covered in Alaska, but one hearing exam and one hearing aid per ear is covered per year in Arizona. This failure to include coverage in plans by insurers has been contested, as Section 1557 of the ACA prohibits discrimination on several grounds, including disability. That provision of the ACA extended the existing nondiscrimination law to all programs and activities that the US Department of Health and Human Services runs or funds, including health insurance marketplaces and plans. And yet a lawsuit from deaf individuals (Schmitt v. Kaiser Foundation Health Plan of Washington) under section 1557, noting that their insurer did not cover hearing aids, was found to be nondiscriminatory because it covered hearing aids for no one—hence arguably was not treating people with hearing loss differently but rather the same.
This disconnect between need for hearing aids and use of them is part of what the new FDA rule is designed to address. The question is whether creating a new OTC hearing aid category will bridge the gap.
How the New OTC Hearing Aid FDA Rule May Benefit People
A major potential benefit of OTC hearing aids are reduced costs. Health and Human Services Secretary Xavier Becerra was asked in August about how OTC hearing aids may impact price; he said the rule “will save consumers on the order of about $1,400 per individual hearing aid or over $2,800 per pair.” These are still just estimates. But the National Institutes of Health and other US agencies feel confident in these estimates, in part due to coordinated research and working groups over the past decade to test how effective technology can be made more cheaply. Recent research has demonstrated that Medicaid eligibility is associated with higher hearing aid use in some groups of older adults in the US, indicating that cost coverage may be an important factor for meaningful access to the technologies. This all reflects that the OTC hearing aid rule, if it results in lower costs as proponents anticipate, could correspondingly increase hearing aid use.
Another major potential benefit of OTC hearing aids is increased geographic accessibility. Allowing consumers to purchase hearing aids directly without a medical provider as an intermediary could address other existing barriers to healthcare. For example, Dr. Planey’s research has found that audiology services are not equally available across the US. In particular, audiologists in the US are not generally located in the communities that need them the most. Their county-level supply and location was negatively correlated with the proportion of older adults reporting hearing difficulties and not found to be correlated with state policies requiring insurance or Medicaid coverage of hearing aids for adults. This finding is matched by studies using other methods, such as recent research examining hearing loss and audiology availability in Appalachia, which reports higher than US-average levels of hearing loss yet does not have increased audiologist availability to match. Similarly, a recent study in Alabama found that over half of adults surveyed did not have access to hearing healthcare due to the distance to a provider, as well as financial constraints.
Making hearing aids available OTC may also increase affordability and accessibility by increasing competition and options. Part of why hearing aids are thought to be so expensive is that only a few companies dominate the market. The Federal Trade Commission (FTC) even filed a formal response to the FDA’s request for comments on the OTC hearing aid rulemaking, supporting the rule and the likely benefits to competition. This was also acknowledged in a statement that President Biden released about the FDA rule back in August, arguing that it will make “our economy more competitive and less concentrated.”
The concern over the small number of hearing aid manufacturers and potential impacts for US consumers is also not new. In 1979 there was a landmark antitrust class action lawsuit against hearing aid manufacturers, where consumers claimed they were forced to pay illegally set higher prices (Reiter v Sonotone Corporation). It went all the way to the Supreme Court, which held that people who bought the hearing aids paid illegally fixed higher prices due to antitrust violations and sustain an injury as a result. That case has shaped antitrust litigation in the US since, as it has led to the consideration of consumer welfare (although the corporation involved in that case tried to argue that the consumers had no standing).
This disconnect between need for hearing aids and use of them is part of what the new FDA rule is designed to address. The question is whether creating a new OTC hearing aid category will bridge the gap.
Potential Limits and Downsides of the New FDA Rule on OTC Hearing Aids
So while there is a lot of potential for the new FDA rule creating OTC hearing aids to lower consumer costs and increase access, it’s important to note what and who is not included in the new rule. This rule covers only hearing aids for mild to moderate hearing loss for adults. It does not cover all hearing aids for all hearing levels, such as individuals with severe hearing loss who may already use hearing aids. The rule also does not impact the previously discussed barriers in insurance or healthcare markets at state and federal levels. The new FDA rule does not expand or include coverage for children, meaning that youth with mild to moderate hearing loss will not qualify for the OTC hearing aids, even though they may medically be able to benefit from the devices. It also does not provide access to audiological services, such as hearing exams that may diagnose hearing loss or fitting services. Additionally, hearing aids are not the only assistive technology that deaf and hard of hearing people may use. For example, some people with hearing loss have or would want a bone-anchored auditory implant or a cochlear implant; the FDA rule does not provide for OTC access to other hearing devices or related services. The rationale in part is that other levels of hearing loss would not be realistic to self-fit and program (like higher amplification) or would require other medical intervention, such as surgery (like cochlear implants). But, as Nitish Pahwa wrote about their unilateral hearing loss and experience with hearing aids, even with these caveats, millions of people stand to benefit from the new rule.
Even for individuals who do qualify though, there are still risks and barriers. This is in part because of hearing aid scams, which are common enough that the FTC has posted guidance about how to avoid them. There is also the possibility that OTC hearing aids could cause more confusion, as consumers may not be aware that some amplification devices are not considered ‘real’ hearing aids or are not FDA approved. For example, when I open my daily local newspaper, multiple ads for devices for hearing loss are being marketed directly to readers. These may look like hearing aids but are in fact ‘personal sound amplification products’ (PSAPs). PSAPs are not considered medical devices and do not amplify as loudly as hearing aids. The FTC has previously settled with such companies that claim to be providing hearing aids or superior solutions for making false or unsubstantiated claims. As of August 2022, the FDA updated its 2009 guidance on the difference between hearing aids and PSAPs to clarify how OTC hearing aids fit in.
For these reasons, several state attorneys’ general have released warning statements about fraudulent OTC hearing aids. As Dr. Virdi’s research on deafness cures in the US since 1860 has demonstrated, doctors and salespeople have developed and promoted hundreds of supposed miracles to cure deafness, often without substantive benefits. There are more recent examples of hearing-related healthcare fraud too, which have resulted in multiple multi-million dollar settlements with the US Department of Justice, including consumers being directed to purchase hearing aids they did not need. This is problematic in multiple senses, as overamplification can itself cause or worsen hearing loss.
This issue is structural and global, as hearing aid dispensers often participate in financial incentive schemes that reward practitioners for device sales. Recent research from Australia found that a majority of hearing aid dispenser audiologists and staff surveyed experienced uncomfortable moral distress over the conflict of interest between financial incentive schemes designed to encourage device sales and the best interests of their clients. Australia currently has a similar patchwork of public programs providing support for hearing aids as in the United States, though they do not make hearing aids available OTC.
…making hearing aids available OTC in the US is a technological solution that may not succeed in achieving increased access and use without addressing underlying social barriers.
These issues reveal a tension that OTC hearing aids may exacerbate—that consumers are on their own to figure out what they need and if it works. Without access to audiologists or other professionals trained in diagnosing hearing loss and customizing hearing technology to match it, people will likely be using self-diagnosis. There are many websites, often run by hearing aid manufacturers, that claim to offer quick DIY tests for assessing one’s hearing. I tried several out while working on this blog. As an adult who may benefit from hearing aids in a state that does not require that they are covered by health insurance and with a family history of hearing loss, I am a prime candidate for OTC hearing aids. While easy and fast to use, the DIY hearing screening results were somewhat confusing and often vague. For example, one concluded that while I likely had hearing loss, I should go to get a test (likely a standard booth test) from a qualified professional, such as an audiologist. But that screening is not covered by the new rule. This is because that is outside the scope of what the FDA regulates, which includes drugs and medical devices not medical care or billing codes. I would have to use my health insurance coverage (if covered) or pay out of pocket for an audiologist appointment.
The online self-screening also did not provide me with an audiogram, a standard chart used in audiology that displays the degree of hearing loss in both ears at different frequencies. This information is critical for appropriate programming of hearing aids. There is a free smartphone screening test from the World Health Organization (hearWHO). The goal of this app is to serve people around the world who may not have access to audiology services in person. A recent examination of this online testing found that almost half the tests were conducted by adults under age 30 and almost half took place on World Hearing Day each year, indicating that this test is not likely reaching the older adults it was intended for, who would be most likely to be experiencing hearing loss.
Finally, making hearing aids available OTC in the US is a technological solution that may not succeed in achieving increased access and use without addressing underlying social barriers. In fact, it could maintain or increase stigma about hearing loss, deafness, and disability. As Dr. Virdi has written, hearing aid marketing may rely on outdated information or negative stereotypes with a promise of passing as hearing. These strategies rely on the fear and stigmatization of deafness and disability. Similarly, Deaf novelist and writer Sara Novic has written about how the claims about health threats from hearing loss may actually stem from ableism and discrimination, not differences in hearing. Fearmongering about disability can lead people to not seeking or wearing hearing aids they need because of stigma. That could mean that OTC hearing aids are not used by some people who may benefit. As Novic has also written, one can support and welcome deaf and hard of hearing people without fearing “a deafer planet.”
Conclusions
OTC hearing aids have the potential to bring much cheaper hearing aids onto the market. Adults currently face many barriers to accessing hearing aids in the US, including high cost, limited or no insurance coverage, and uneven availability of medical professionals to prescribe and support them. Allowing companies to sell OTC hearing aids directly to consumers may increase who and where hearing aids are sold, which federal agencies hope, in turn, will improve competition and incentivize lower costs. Combined, this could reduce the gap between the number of adults with mild to moderate hearing loss who would like a hearing aid and those who are using them. However, there are potential downsides and limitations to this policy. In particular, there are still many people, including adults with more significant levels of hearing loss and children of all hearing levels, who will not substantively benefit from the new rule. They remain uncovered or partially covered by a patchwork of state and federal laws and plans, such as the wide variability in what states require for essentially health benefits in private insurance or what states cover in Medicaid plans. These are areas of potential further policy intervention to provide the benefits of hearing aids, and broader hearing-related healthcare, to even more US residents.
ABOUT THE AUTHOR
Kaitlin Stack Whitney is a fellow at the Rockefeller Institute of Government and an assistant professor in the Science, Technology & Society Department at the Rochester Institute of Technology.