
In 1970, Congress passed the Controlled Substances Act, which created the modern federal scheduling system for drugs, based on their respective risk profile and medical applications. The lower the schedule on a scale of I to V, the more dangerous the drug is presumed to be. Those substances that were determined to have a high potential for abuse and no currently accepted medical value were designated as Schedule I drugs (ex., heroin, LSD); while Schedule V drugs are seen as the least dangerous, displaying the lowest potential of abuse or dependence (ex., cough and cold medications with low amounts of codeine). Substances can be added, removed, or reclassified within the scheduling. For example, the Trump administration is determining whether to reschedule cannabis from a Schedule I drug to a Schedule III drug. However, while cannabis may be moving to a less restrictive category, increasing public health concerns about derivatives of another drug—kratom—have prompted executive and legislative action at the federal, state, and local levels in the opposite direction.
What is Kratom?
Kratom is a tropical tree native to Southeast Asia. The kratom leaves contain two compounds, mitragynine and the more powerful 7-hydromitragynine (7-OH), that can have stimulant-like effects in low doses and opioid-like effects in higher doses, as well as an increased chance of dependency. In the most severe cases, consumption of kratom products can result in liver toxicity, seizures, substance-use disorder, and death. Originally consumed by chewing on the leaves or brewed in teas as a source of pain relief, kratom and its compounds can now be found in powders, energy drinks, vapes, herbal supplements, and gummies. While the raw kratom leaves have limited concentrations of both compounds, with mitragynine being more prevalent than 7-OH, companies have begun to concentrate or synthetically produce 7-OH to create stronger products. Kratom and its derivatives are not currently scheduled substances, and the US Food and Drug Administration (FDA) has not approved kratom, 7-OH, or mitragynine for use in prescription or over-the-counter drugs. However, the availability of kratom products online and in vape shops and convenience stores means that many people may consume the products without awareness of the potential health risks or questionable medical claims. The 2021 National Survey on Drug Use and Health estimated that approximately 1.7 million people had used kratom in the last year, though a policy brief by the American Kratom Association, put out in the same year, found that between 11 and 16 million Americans consume kratom products.
How Are Governments Responding?
Federal
In July 2025, the FDA announced that, because of public health concerns, they were recommending to the US Drug Enforcement Administration (DEA) that the 7-OH compound—not the kratom plant—should be scheduled as a Schedule I controlled substance. The FDA additionally released a report that assessed the scientific data related to 7-OH and its usage. The report found that the “pharmacological profile, abuse liability, and emerging patterns of non-medical use establish 7-OH as a dangerous substance. Current regulatory gaps have enabled widespread availability of these products despite their opioid-like properties and necessitate immediate policy intervention to address this emerging threat to American public health.” FDA Commissioner Dr. Marty Makary told reporters, “This may be the fourth wave of the opioid epidemic. Concentrated, synthetic 7-OH may be the fourth wave of the opioid epidemic.”
Traditionally, the DEA has scheduled controlled substances in a two-step process. First, issuing a temporary scheduling order and then promulgating permanent scheduling through the rulemaking process. However, the temporary scheduling is not a required step, and the DEA could choose to proceed directly to permanent scheduling. That would involve the DEA doing their own review into 7-OH’s abuse potential, medical use, and safety. The DEA would also consult with the US Department of Health and Human Services (HHS). A proposed rule would be published in the Federal Register, and a period for public comment would be determined. If 7-OH becomes a Schedule I drug, the manufacturing, distribution, and possession of 7-OH products would become illegal.
This would not be the first time that the federal government has explored scheduling kratom and its derivatives. In 2016, the DEA announced its intention to schedule mitragynine and 7-OH as Schedule I drugs. A rule creating the temporary scheduling was posted, but there was public backlash against the action. Advocacy groups organized demonstrations, phone calls to Congress, and petitions decrying the scheduling attempt and citing the benefits of kratom as an opioid alternative to managing pain. The reaction was strong enough that the DEA reconsidered the proposal and withdrew the temporary scheduling.
States
While the federal government contemplates scheduling 7-OH, several states have also recently taken action to regulate kratom and its derivatives on a number of different fronts.
Kratom Bans and Restrictions by State
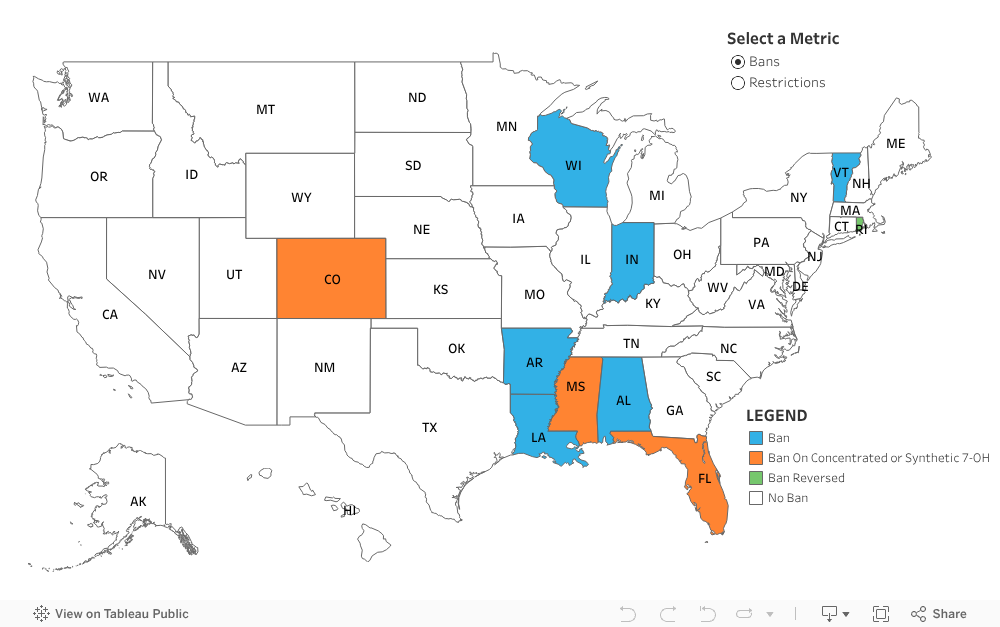
Bans
In August 2025, Florida Attorney General James Uthemeir issued an emergency rule that schedules 7-OH as a Schedule I substance in the state. The rule will apply to 7-OH concentrates, not the 7-OH that can be found naturally in kratom leaves. 7-OH concentrates were therein immediately illegal to sell, possess, or distribute in Florida. Since the ban, the state has reported the removal of more than 17,000 packages of concentrated 7-OH. Effective August 1, 2025, Louisiana also added 7-OH and mitragynine to Schedule I for the state. Mississippi and Colorado also banned synthetic 7-OH in 2025. Alabama, Arkansas, Indiana, Vermont, and Wisconsin all previously banned kratom or its derivatives, 7-OH or mitragynine. Rhode Island recently became the first state to reverse its ban; though still currently illegal under the state ban, the state is creating a regulatory framework for the manufacture and sale of kratom, similar to the state’s cannabis program, to be effective April 2026.
{kind=link}
Age Restrictions
In July 2025, Mississippi became the latest state to enact an age restriction for the purchase of kratom products. Mississippi residents must now be 21 years old to make kratom purchases. Colorado, Florida, Georgia, Kentucky, Maryland, Oregon, South Dakota, Tennessee, Virginia, and West Virginia all similarly have restricted sales to those 21 years of age or older. Arizona, Illinois, Minnesota, Nevada, Oklahoma, Texas, and Utah have all restricted sales to those 18 years old or older. Additionally, several other states have introduced legislation to set age restrictions on kratom products. New York’s legislature has passed legislation that would restrict sales of kratom products to those 21 years old or older, but the legislation has not yet been signed by the governor.
Local Government
Adding another level of regulation, some local municipalities have also imposed bans on kratom in states where there are currently no restrictions. Orange County, California, banned synthetic kratom products in August 2025. Newport Beach, California, banned the sale or distribution of kratom in 2024, joining San Diego and Oceanside. Bans have also been passed at the local level in states where age restrictions on kratom have been enacted, going further than the state law. In New Hampshire, Franklin was the first municipality to pass a ban. Illinois has several local governments that have prohibited kratom, including Alton, Jerseyville, Marion, Herrin, and Godfrey. While the restrictions on kratom are limited to these local jurisdictions, it further adds to the uncertainty and inconsistency in kratom regulations.
Conclusion
This fractured approach, in the absence of federal scheduling thus far, has created significant variation in how kratom is regulated depending on where a person lives. In some communities, consumers can freely purchase kratom in smoke shops or online, while in others, possession can result in criminal penalties. The ongoing debate reflects broader tensions in US drug policy: how to balance harm reduction, public health, and individual choice in the face of substances with both risks and reported therapeutic potential. Action at the federal level would provide guidance and minimize the patchwork of regulations that are currently in place at the state and local levels.
ABOUT THE AUTHOR
Heather Trela is the director of operations and a fellow at the Rockefeller Institute of Government